
GLOW vs. KLOW
| Compare | KLOW | GLOW |
|---|---|---|
| Vial size | 80 mg | 70 mg |
| Compounds | GHK-Cu + BPC-157 + TB-4 + KPV | GHK-Cu + BPC-157 + TB-4 |
| Standard dose | 3.2 mg | 2.8 mg |
| Standard draw | 10 units after 2.5 mL BAC water | 10 units after 2.5 mL BAC water |
| Frequency | Daily -> 5x per week -> 2-3x per week | Daily -> 5x per week -> 2-3x per week |
| Best fit | Reactive or inflammation-driven skin | Firmness, fine lines, texture |
GLOW contains GHK-Cu, BPC-157, and Thymosin Beta-4. KLOW contains GHK-Cu, BPC-157, Thymosin Beta-4, and KPV. The standard KLOW and GLOW protocols use identical GHK-Cu, BPC-157, and TB-4 doses, a 10-unit standard draw, and a 12-week schedule. KPV adds inflammation control. It does not change the basic dosing cadence.
No controlled trial has compared GLOW with KLOW.
GLOW & KLOW benefits
| Benefit | GLOW | KLOW |
|---|---|---|
| Firmness and elasticity | ✓ | ✓ |
| Reducing fine lines | ✓ | ✓ |
| Scar remodeling | ✓ | ✓ |
| Improving texture and general skin quality | ✓ | ✓ |
| Rosacea-pattern inflammation | — | ✓ |
| Reactive or flushing-prone skin | — | ✓ |
| Post-procedure redness | — | ✓ |
| Inflammatory acne | — | ✓ |
KLOW can be used as a stand-in for GLOW — adding KPV does not detract from the shared benefits — but is uniquely suitable when inflammation is part of the skin baseline. KLOW and GLOW can be switched during a cycle because GHK-Cu, BPC-157, and TB-4 use identical per-injection amounts in each stack. If inflammation is a baseline issue, beginning with KLOW for the activation phase (weeks 1-4) is critical to calm reactive skin and provide the environment needed for remodeling. The total dose changes from 3.2 mg with KLOW to 2.8 mg with GLOW because KLOW includes 400 mcg KPV.
GLOW & KLOW Peptides
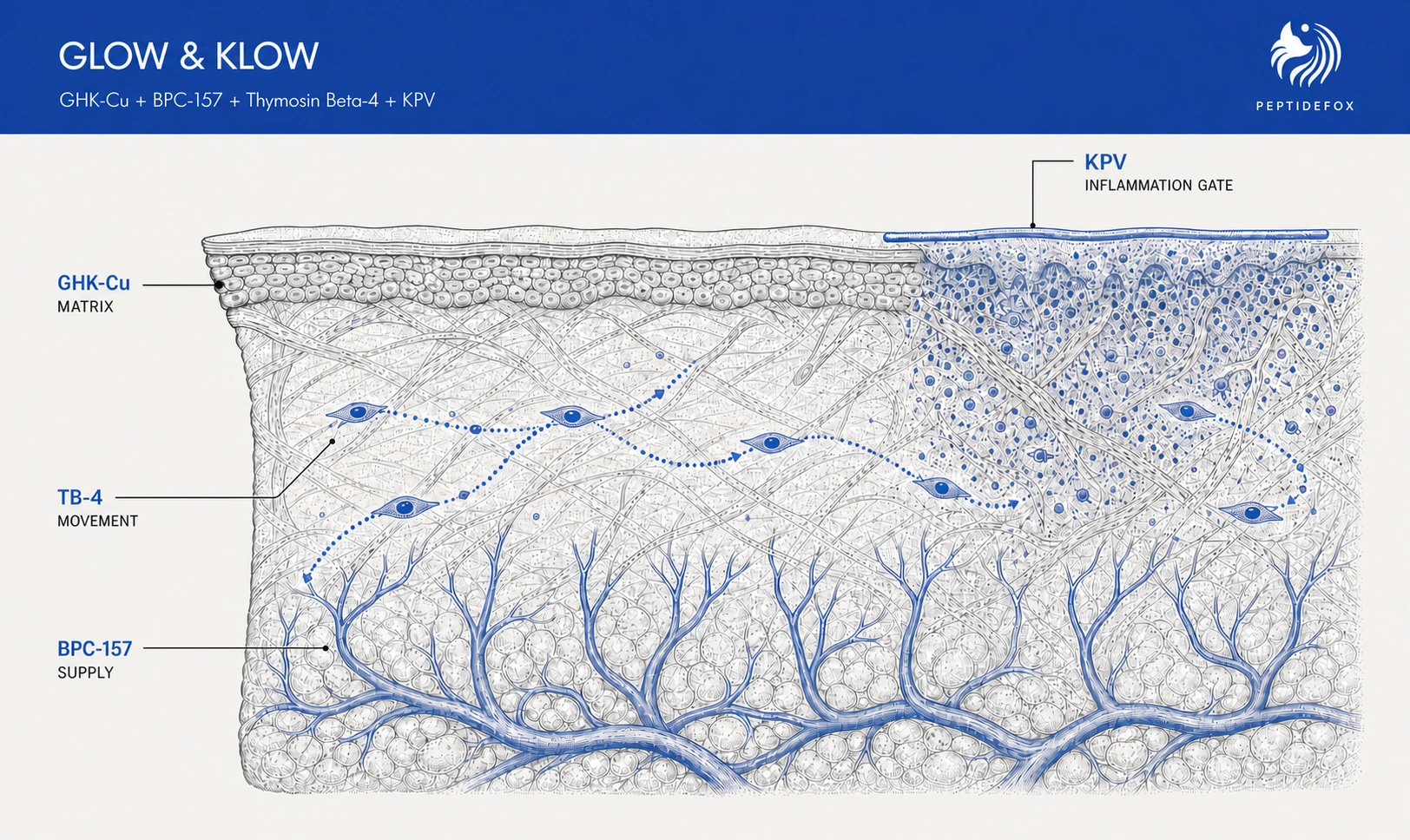
GLOW and KLOW are pre-mixed peptide blends of GHK-Cu, BPC-157, Thymosin Beta-4, and KPV (KLOW only). Each compound included in the blends addresses a specific bottleneck as skin repair slows with age across several connected systems:
- GHK-Cu shifts skin cells toward making and organizing new collagen, while its copper supports the cross-linking that gives the matrix strength.¹
- BPC-157 supports the blood-vessel layer of repair, improving the capillary supply that brings oxygen and nutrients into active tissue.²
- Thymosin Beta-4 helps repair cells reach damaged tissue and organize the rebuilding process by keeping actin available for cell movement.³
- KPV (KLOW only) limits persistent inflammatory signaling so it does not keep interfering with the repair work of GHK-Cu, BPC-157, and TB-4.⁴
Each compound handles a different job and has its own mechanistic rationale. However, no study has tested the specific GHK-Cu-heavy ratios or evaluated GLOW or KLOW in a controlled setting.
Peptide blends are designed primarily to reduce injection burden and improve protocol compliance — rather than three or four separate injections to manage, there is simply one. Convenience has a trade-off: the fixed ratio cannot optimize the dose and frequency of each compound or allow one compound to be adjusted without changing the others.
GHK-Cu: collagen building and repair
What it is
GHK-Cu is a three-amino-acid peptide bound to copper. It carries copper into the repair processes that build and organize the skin’s structural matrix.
How it works
GHK-Cu changes which repair instructions skin cells follow, increasing collagen, elastin, and antioxidant production while helping clear damaged tissue. Its copper also supports lysyl oxidase, the enzyme that cross-links new collagen fibers and gives the matrix strength (gene regulation, tissue clearing, and collagen cross-linking¹).
Benefits for skincare
GHK-Cu addresses both sides of skin remodeling: removing damaged matrix and building its replacement. The practical targets are firmness, elasticity, finer texture, and more organized remodeling of scarred or sun-damaged tissue.
Evidence
Gene-expression and wound-healing research support the matrix-remodeling mechanism. Small human cosmetic-skin studies report changes in wrinkle depth and skin density, but the strongest human evidence is topical; it does not establish how much injected GLOW or KLOW changes human skin.¹
Regulatory status
GHK-Cu was not part of the July 23–24, 2026 PCAC review. FDA currently places non-injectable GHK-Cu in Category 1 while it remains under evaluation, but treats injectable GHK-Cu separately because of route-specific safety and product-quality questions.⁸
Injectable GHK-Cu was moved to Category 2 in September 2023 and will return to PCAC for a vote before the end of February 2027. On February 27, 2026, HHS Secretary Robert F. Kennedy Jr. said GHK-Cu was among approximately 14 peptides expected to return to Category 1. If completed, that change would restore the compounding pathway for injectable GHK-Cu; it would not constitute FDA approval.¹⁰
BPC-157: blood supply to the repair area
What it is
BPC-157 is a synthetic 15-amino-acid peptide modeled from a protective protein fragment found in gastric juice. Its role in GLOW and KLOW is to support the blood supply behind tissue repair, rather than build collagen directly.
How it works
BPC-157 signals blood-vessel cells to relax existing vessels, move into damaged tissue, and form new capillaries. In tendon repair cells, it also increased the number of places where growth hormone can attach; it made the cells more responsive when growth hormone was present without activating the signal on its own (new blood vessel formation²).
Benefits for skincare
Active skin remodeling needs oxygen, nutrients, and a route for repair cells to reach the area. BPC-157 supports that supply layer so oxygen and nutrients can reach the tissue while GHK-Cu and TB-4 do their repair work.
Evidence
Cell and animal models support BPC-157's blood-vessel signaling and repair-cell effects. Human evidence remains thin and uncontrolled, and no human study shows that SubQ BPC-157 builds new capillaries in skin or improves a GLOW or KLOW outcome.²
Regulatory status
BPC-157 does not have an FDA-approved therapeutic indication. On July 23, 2026, PCAC voted 8–6 to recommend adding BPC-157 free base and acetate to the 503A Bulk Drug Substances List. Final FDA action is still pending; the recommendation concerns compounding access, not therapeutic approval or proof of efficacy.⁸
Thymosin Beta-4: repair-cell movement and tissue organization
What it is
TB-4 is a naturally occurring 43-amino-acid peptide involved in cell movement and tissue repair. It is not the same molecule as TB-500, the shorter 17–23 fragment, even when product labels use the names interchangeably.⁷
How it works
Repair cells move by building and releasing an internal scaffold made from actin. TB-4 holds loose actin in reserve so the scaffold can be assembled where it is needed. TB-4 can also release Ac-SDKP, a smaller peptide studied for anti-scarring and anti-inflammatory effects (actin sequestration and Ac-SDKP release³).
Benefits for skincare
TB-4 supports the movement of repair cells through damaged tissue and the organization of the rebuilding process. Its role complements GHK-Cu: TB-4 helps position the repair cells, while GHK-Cu handles more of the matrix-building work.
Evidence
TB-4 has human clinical research across corneal, cardiac, and wound-repair programs, plus dermal wound-healing models. Those studies support the broader repair mechanism, not the efficacy of a 400 mcg SubQ dose in GLOW or KLOW, and their findings cannot be assigned to a TB-500 fragment vial.³ ⁶ ⁷ ⁹
Regulatory status
TB-4 remains investigational in the United States. The July 23 PCAC review and 8–6 recommendation covered TB-500 free base and acetate, not TB-4, so that update cannot be treated as a regulatory change for the TB-4 used in GLOW and KLOW.⁸ ⁹
KPV: the inflammation switch in KLOW
What it is
KPV is a three-amino-acid fragment of alpha-MSH and the only compound unique to KLOW. Its job is to control persistent inflammatory signaling rather than add another matrix-building signal.
How it works
KPV blocks the inflammation switch from reaching the cell nucleus, lowering production of inflammatory molecules (NF-kB signaling⁴). This does not eliminate the early inflammation needed to start repair; it is intended to stop persistent signaling from continuing to break down tissue.
Benefits for skincare
KPV gives KLOW a dedicated inflammation-control layer for rosacea-pattern, flushing-prone, post-procedure, or otherwise reactive skin. It helps keep inflammation from overwhelming the GHK-Cu, BPC-157, and TB-4 repair work.
Evidence
KPV’s anti-inflammatory evidence comes from cell and animal models. Its strongest route-specific evidence uses oral delivery into PepT1-rich inflamed gut tissue; that does not establish what SubQ KPV does in human skin, and no controlled human KPV trial has measured a skincare outcome.⁴ ⁵
Regulatory status
KPV does not have an FDA-approved therapeutic indication. On July 23, 2026, PCAC voted 8–6 to recommend adding KPV free base and acetate to the 503A Bulk Drug Substances List. Final FDA action is still pending. If FDA follows the recommendation, it would change how KPV may be compounded; it would not create human efficacy data.⁸
GLOW Peptide
GLOW is a pre-mixed blend of GHK-Cu, BPC-157, and TB-4 in a fixed ratio:
- GHK-Cu rebuilds collagen and clears damaged tissue.¹
- BPC-157 supports the capillary supply feeding the repair area.²
- TB-4 moves repair cells into position and supports organized healing.³
GLOW is the skincare stack for collagen rebuilding, capillary support, and organized cell migration.
GLOW peptide dosage
A standard GLOW-70 vial contains 50 mg GHK-Cu, 10 mg BPC-157, and 10 mg TB-4. Every draw keeps that fixed 50/10/10 ratio.
- Low Dose: 1.4 mg total (1 mg GHK-Cu + 200 mcg BPC-157 + 200 mcg TB-4)
- Standard Dose: 2.8 mg total (2 mg GHK-Cu + 400 mcg BPC-157 + 400 mcg TB-4)
- Elevated Dose: 4.2 mg total (3 mg GHK-Cu + 600 mcg BPC-157 + 600 mcg TB-4)
For a GLOW-70 vial reconstituted with 2.5 mL of BAC water:
- Low Dose: 5 units
- Standard Dose: 10 units
- Elevated Dose: 15 units
The standard GLOW dose per day is 2.8 mg, but daily dosing only applies to the activation phase in weeks 1–4. GLOW has no trial-established dose that combines the three compounds. The GLOW dosage calculator solves BAC water and syringe units for a different vial or dose.
KLOW Peptide
KLOW is a pre-mixed blend of GHK-Cu, BPC-157, TB-4, and KPV in a fixed ratio:
- GHK-Cu rebuilds collagen and clears damaged tissue.¹
- BPC-157 supports the capillary supply feeding the repair area.²
- TB-4 moves repair cells into position and supports organized healing.³
- KPV pre-empts the inflammation switch before it activates.⁴
KPV is what distinguishes KLOW from GLOW. It makes KLOW the inflammation-focused stack for reactive skin.
KLOW peptide dosage
A standard KLOW-80 vial contains 50 mg GHK-Cu and 10 mg each of BPC-157, TB-4, and KPV. Every draw keeps that fixed 50/10/10/10 ratio.
- Low Dose: 1.6 mg total (1 mg GHK-Cu + 200 mcg each of BPC-157, TB-4, and KPV)
- Standard Dose: 3.2 mg total (2 mg GHK-Cu + 400 mcg each of BPC-157, TB-4, and KPV)
- Elevated Dose: 4.8 mg total (3 mg GHK-Cu + 600 mcg each of BPC-157, TB-4, and KPV)
For a KLOW-80 vial reconstituted with 2.5 mL of BAC water:
- Low Dose: 5 units
- Standard Dose: 10 units
- Elevated Dose: 15 units
The standard KLOW dose per day is 3.2 mg, but daily dosing only applies to the activation phase in weeks 1–4. No controlled KLOW trial has established the 1.6–4.8 mg dose range. The KLOW dosage calculator solves BAC water and syringe units for a different vial mix or dose.
GLOW & KLOW Protocols
The three-phase structure changes what the protocol is trying to accomplish across the 12-week cycle. It is a mechanistic framework for sequencing repair, not a phase model established in a controlled GLOW or KLOW trial.
Phase 1: Activation (Weeks 1–4)
Activation establishes the repair environment. GHK-Cu shifts skin cells toward producing new collagen and supplies copper for structural cross-linking. BPC-157 supports the small-vessel network feeding active tissue. TB-4 helps repair cells move into position and organize the rebuilding process. KLOW adds KPV to reduce persistent inflammatory interference.¹ ² ³ ⁴
What to expect
Around week 2, the working expectation is improved hydration, less redness — particularly with KLOW — and smoother texture as collagen-building signals and vascular support come online.
Phase 2: Remodeling (Weeks 5–8)
Remodeling is the sustained matrix-building phase. GHK-Cu supports collagen, elastin, and other components of the skin matrix while BPC-157 maintains the capillary supply and TB-4 coordinates repair-cell movement.¹ ² ³
What to expect
Weeks 4–6 are when fine lines may begin to soften, elasticity may improve, and tone may even.
Phase 3: Maintenance (Weeks 9–12)
Maintenance shifts from intensive rebuilding toward consolidating collagen quality as the newly formed matrix continues to organize and cross-link. A 4–8-week break follows week 12 before another intensive cycle.
What to expect
Across weeks 8–10, the expected emphasis shifts toward matrix remodeling and integration: pores may appear more refined, visible glow may increase, and skin may feel denser. By week 12 and beyond, the target is stable skin density and sustained firmness rather than continued week-to-week visible change.
These checkpoints are protocol expectations, not trial-established timelines. The human cosmetic studies cited for GHK-Cu used topical formulations over 12 weeks; they do not establish the timing or magnitude of outcomes from injected GLOW or KLOW.¹
GLOW Peptide Protocol
The GLOW skincare protocol also runs for 12 weeks. The 2.8 mg dose stays fixed while frequency falls:
- Activation (weeks 1–4): 2.8 mg daily
- Remodeling (weeks 5–8): 2.8 mg 5x per week
- Maintenance (weeks 9–12): 2.8 mg 2-3x per week
- After week 12: 4–8 weeks off
At the standard dose, one GLOW-70 vial contains 25 injections:
- The full schedule uses 56–60 injections.
- The standard protocol requires three GLOW-70 vials.
- The elevated dose requires four vials.
- The low dose still requires three vials to stay within the 28-day refrigerated-use window.
No controlled GLOW trial has tested this schedule or established 12 weeks as the optimal cycle length.
KLOW Peptide Protocol
The KLOW skincare protocol runs for 12 weeks across activation, remodeling, and maintenance. The 3.2 mg dose stays fixed while frequency falls:
- Activation (weeks 1–4): 3.2 mg daily
- Remodeling (weeks 5–8): 3.2 mg 5x per week
- Maintenance (weeks 9–12): 3.2 mg 2-3x per week
- After week 12: 4–8 weeks off
At the standard dose, one KLOW-80 vial contains 25 injections:
- The full schedule uses 56–60 injections.
- The standard KLOW protocol requires three 80 mg vials.
- The elevated dose requires four vials.
- The low dose still requires three vials to stay within the 28-day refrigerated-use window.
No controlled KLOW trial has tested this schedule or established 12 weeks as the optimal cycle length.
Side Effects and Safety
The most common reported effect is a 30–60-second sting from the copper-peptide complex. Less common reports include fatigue 12–24 hours after dosing, injection-site redness, and brief flushing. The blue vial color is expected.
More BAC water lowers concentration; slow injection and site rotation may reduce local irritation.
The main KLOW and GLOW exclusions and caution flags are:
- Active cancer or cancer history: excluded during active cancer treatment; cancer treatment or remission within the past five years requires explicit clearance and ongoing supervision from the clinician managing that history.
- Wilson’s disease or copper overload: contraindicated with copper-handling disorders.
- Pregnancy or breastfeeding: no pregnancy or breastfeeding safety data exist for KLOW or GLOW.
- Recent surgery: use is generally deferred for at least two weeks after major surgery.
- WADA-tested athletes: TB-4 is on the prohibited list.
No controlled trial has measured side-effect rates for a complete KLOW or GLOW blend.
Frequently Asked Questions
How do you reconstitute GLOW / KLOW?
- Prepare a clean work area. Gather the sealed blend vial, BAC water, a sterile syringe with a fresh needle, and alcohol swabs.
- Sanitize the blend and BAC water vials. Wipe each rubber stopper with a fresh alcohol swab and let the alcohol dry.
- Draw the BAC water. Slowly draw the exact water volume and tap out any air bubbles.
- Add the water slowly. Let the BAC water run down the inside vial wall instead of forcing it onto the powder.
- Dissolve the powder. Swirl or roll the vial gently. Do not shake.
- Label and refrigerate. Record the date and concentration, then store at 2–8°C away from direct light.
Use the peptide reconstitution guide for the full handling sequence.
Does KLOW peptide dosage differ for women?
KLOW does not use a separate female dose. Each injection remains 1.6–4.8 mg total; the standard KLOW dose for women is 3.2 mg per injection (2 mg GHK-Cu plus 0.4 mg each of BPC-157, TB-4, and KPV).
Where do you inject GLOW / KLOW?
GLOW and KLOW are injected subcutaneously in a rotated site. The abdomen, thigh, and lateral hip all work; rotation reduces repeated local irritation. See where to inject peptides for the full anatomical breakdown.
What if you miss a dose?
A missed dose is skipped instead of doubled. The next injection stays on the scheduled dose and cadence.
Why are GLOW and KLOW blue?
KLOW and GLOW are blue because most of each vial is GHK-Cu, a peptide bound to copper. A clear blue solution is expected; cloudiness, particles, or loss of the blue tint are reasons to discard the vial.
Is KLOW a weight-loss peptide?
No. KLOW is a skincare stack built around collagen, blood supply, repair-cell movement, and inflammation control. It has not been shown to cause weight loss.
How are GLOW & KLOW different from the Wolverine Stack?
GLOW and KLOW are skincare stacks. Their standard doses contain 400 mcg of TB-4. The Wolverine Stack and Injury Recovery Protocol use 2–4 mg of TB-4 or TB-500 per injection. That range comes from equine practice, not human dose-finding.
How does injection timing affect GLOW / KLOW protocols?
Morning and evening dosing both work for KLOW and GLOW; consistency across scheduled dosing days matters more than the hour of injection.
Can GLOW / KLOW be assembled from separate peptide vials?
KLOW and GLOW can be assembled from separate peptide vials. Sourcing and reconstituting each compound separately allows independent dosing but adds cold-chain items and sterile draws. A premixed KLOW or GLOW vial fixes the ratio and reduces handling.
How long does it take GLOW or KLOW to work?
No controlled GLOW or KLOW trial establishes a results timeline. Texture, fine lines, redness, and firmness change gradually, so baseline photographs provide a more reliable comparison than day-to-day observation.
Related Topics
- KLOW Dosage Calculator — KLOW concentration and syringe-unit math
- GLOW Dosage Calculator — GLOW concentration and syringe-unit math
- KPV Guide — KPV mechanism and use cases
- GHK-Cu for Skin — GHK-Cu mechanism and skin context
- BPC-157 Guide — BPC-157 evidence and dosing
- TB-500 Guide — TB-4 and TB-500 identity
- Where to Inject Peptides — subcutaneous injection sites
- Peptide Reconstitution Guide — vial handling and mixing technique
References
¹ GHK-Cu gene modulation — COL1A1/COL3A1 collagen gene activation, lysyl oxidase cross-linking, bidirectional MMP regulation, SOD/catalase antioxidant expression, and broad gene modulation: Pickart L, Margolina A. Int J Mol Sci 2018. DOI: 10.3390/ijms19071987; Pickart L. J Biomater Sci Polym Ed 2008. PubMed: 18644225
² BPC-157 blood vessel signaling — Src-caveolin-1-eNOS signaling, nitric oxide release, ERK1/2-c-Fos/c-Jun/Egr-1-VEGF-a signaling, and growth-hormone receptor expression in cell and animal models: Hsieh MJ et al. Sci Rep 2020. DOI: 10.1038/s41598-020-74022-y; Huang T et al. Drug Des Devel Ther 2015. DOI: 10.2147/DDDT.S82030; Chang CH et al. Molecules 2014. PMC6271067; He L et al. Front Pharmacol 2022. PMC9794587
³ Thymosin beta-4 tissue repair and structure — G-actin sequestration, cytoskeletal organization, and the meprin-α/prolyl oligopeptidase pathway that releases Ac-SDKP from TB-4: Goldstein AL et al. Trends Mol Med 2005. PubMed: 16099219; Xue B et al. Proc Natl Acad Sci 2014. PMC4217450; Kumar N et al. Am J Physiol Renal Physiol 2016. DOI: 10.1152/ajprenal.00562.2015
⁴ KPV anti-inflammatory mechanism — NF-κB-related signaling, cytokine suppression, and immune-cell effects in cellular and animal models: Luger TA, Brzoska T. Ann Rheum Dis 2007. PubMed: 17921186; Getting SJ, Schiöth HB, Perretti M. J Pharmacol Exp Ther 2003. PubMed: 12750433
⁵ KPV oral delivery via PepT1 — transporter uptake and inflammatory signaling in murine intestinal models: Kannengiesser K et al. J Crohns Colitis 2008. PubMed: 21172189; Dalmasso G et al. Gastroenterology 2008. PMC2431115; Viennois E et al. Cell Mol Gastroenterol Hepatol 2016. PMC4957955
⁶ TB-4 wound healing — dermal repair acceleration with TB-4 in wound models: Malinda KM et al. J Invest Dermatol 1999. PubMed: 10469299
⁷ TB-500 molecular identity — TB-500 is the synthetic acetylated 17–23 fragment of thymosin beta-4, Ac-LKKTETQ, and is distinct from 43-amino-acid TB-4: Esposito M et al. Drug Test Anal 2012. PubMed: 22962027
⁸ FDA compounding-pathway status — current 503A classification for GHK-Cu, the July 23–24, 2026 PCAC agenda for BPC-157, KPV, and TB-500, and FDA’s route-specific compounding concerns: FDA 503A bulk drug substances update; July 23–24, 2026 PCAC meeting; FDA safety-risk list
⁹ TB-4 investigational program — RGN-259 clinical investigation for neurotrophic keratopathy: ClinicalTrials.gov NCT02600429
¹⁰ HHS Category 1 update — On February 27, 2026, HHS Secretary Robert F. Kennedy Jr. announced that GHK-Cu was among approximately 14 peptides expected to return to Category 1. FDA has scheduled GHK-Cu for PCAC consideration before the end of February 2027: FDA PCAC meeting
Medical Disclaimer
The content in this protocol guide is for informational purposes only and does not constitute medical advice. Always consult with a qualified healthcare provider before beginning any new protocol, supplement, or medication.